The second day of the House of Lords Committee stage on the Mental Capacity (Amendment) Bill took place on Monday 15th October. You can read the Hansard transcript of the debate online. The face of the Bill has not yet been amended, despite many possible amendments being debated. In this blog, I set out some of the good news from this debate, challenge some interesting interpretations of our current mental capacity law, and rant about reflect on the Government’s intransigence on the question of the appropriate role for care home managers.
Some Good News
The Government have committed to three important and positive changes to the Bill:
- Including 16 and 17 year olds in the Liberty Protection Safeguards;
- Ensuring that the Bill reflects the need to consult the cared-for person and that their wishes and feelings are at the heart of the scheme; and
- Changing the language of “unsound mind”, which is entirely out of step with contemporary approaches to intellectual disability.
This is all good news. Whilst it is probably churlish of me to point this out, the Bill and the debates on it would all have been much better if these important elements had been included on the face of the Bill as introduced. However, positive progress is to be applauded, and those who raised these issues through second reading and in the first committee day can consider these (especially 1 and 3) as positive wins.
Interesting Interpretations
I am less certain about the second commitment from the Government, to consult the cared-for person. In part, I am reserving judgement until I can see the detail of the amendments that the Government propose to bring this into being. Those who know the proposals from the Law Commission of England and Wales will remember that they proposed somewhat wider changes to the place of the person in our Mental Capacity Act 2005 (MCA) than my (perhaps minimalist) interpretation of the statement from Lord O’Shaugnessy would suggest.
In their 2017 Report, the Law Commission proposed amending section 4 of the MCA so that P (the person with impaired capacity)’s wishes and feelings are prioritised in all best interests decision-making (this would, of course, include deprivation of liberty decision-making). If, as I would expect, the current Bill only changes the list of people to be consulted under Paragraph 17 of Schedule AA1 to include P, then we will get a significantly watered-down version of the proposal for respecting P’s wishes and feelings. As a result, we will miss out on the opportunity to bring English law closer into line with Article 12 of the UN Convention on the Rights of Persons with Disabilities. Part of the problem here is, I think, as a result of some ‘interesting’ interpretations of our current MCA.
According to Lord O’Shaugnessy:
As I am sure noble Lords know, supported decision-making is already part of the law, and indeed it is the second principle of the Mental Capacity Act. … It is already the case that steps should be taken to support people to make their own decisions. We have not brought forward the Law Commission’s recommendation to set up a formal supported decision-making scheme because that legal entitlement already exists. Wherever possible, of course, people should make decisions for themselves and be supported to do so. (Col 348)
This interpretation of the MCA is ‘interesting’ to me for three reasons:
- It suggests that having principle 2 as part of the current law means that supported decision-making happens in practice;
- It suggests that principle 2 of the MCA carries over into best interests decision-making; and
- It suggests that the MCA already includes a formal supported decision-making scheme.
As regular readers of this blog and my wider academic work will know, I have spent the last several years working on this issue. I would like to offer an alternative interpretation of the current impact and extent of principle 2 of the MCA.
The Everyday Decisions research project investigated how supported decision-making happens in practice in England and Wales. We interviewed 25 care professionals and 15 disabled people about their experiences of, and approaches to supported decision-making. We found that supported decision-making was well embedded in practice when used to support everyday choices about what to wear, what to eat, or what to do. In contrast, decisions about wider life choices (education, employment, housing) and more complex decisions like consenting to medical treatment, managing personal finances, making wills or granting Lasting Powers of Attorney were not so well supported. Instead, in relation to these kinds of decisions, care and support professionals were more inclined to consider them to be ‘too difficult’ and to fall back on an expansive interpretation of the best interests powers under the MCA. Please see the project report for more detail on these findings.
Official reviews of the MCA, including the House of Lords Select Committee Post-Legislative Scrutiny Report from 2014 have also found that the current approach to supported decision-making under principle 2 does not always work well in practice (see, especially, paragraphs 79-83).
In terms of the technical, doctrinal, extent of supported decision-making under principle 2 of the MCA, it is important to look at how principle 2 is framed in legislation. The full text of principle 2 is “A person is not to be treated as unable to make a decision unless all practicable steps to help him to do so have been taken without success.” (MCA, s. 1(3)). Principle 2 does not set out a right to supported decision-making, nor does it provide a formal scheme for supported decision-making. Instead, it sets out that a person is not to be considered “unable to make a decision” (in other words to lack capacity) unless “all practicable steps to help him do so have been taken without success”. Principle 2, refers to support to make a decision, not to support towards expressing a view on a best interests decision.
Respect for the person’s wishes and feelings under the MCA was somewhat expanded by the Supreme Court decision in Aintree University Hospitals NHS Foundation Trust v James [2013] UKSC 67. In that case Lady Hale stated that “the purpose of the best interests test is to consider matters from the patient’s point of view”. This has shifted the legal interpretation of best interests to include more engagement with P’s wishes and feelings, but this is absolutely not the same as a formal right to supported decision-making, nor is it a legal entitlement to supported decision-making. At present, at best, principle 2 of the MCA offers informal recognition of the need to offer support, especially around communication, to help people to make their own decisions where possible. This is not, of course, to belittle the very important potential of principle 2 if it were to be fully implemented in practice.
In contrast, formal supported decision-making schemes do exist in several countries around the world (including in Canada, Australia, Sweden, Ireland and, most recently, Peru). These schemes offer graded support frameworks ranging from informal support (like that in the MCA) through to appointed and formally supervised supporters and co-decision-makers. There is not space to cover these in detail in this (already long!) blog, but I will add a link to more information when possible. The oldest of these frameworks, the Swedish model of the ‘godman’ or mentor has been around for more than half a century. The framework in British Columbia, Canada, has been in force since 1996. The frameworks in Australia, other Canadian provinces, Ireland and Peru are much more recent and are designed to bring those jurisdictions into line with disabled people’s rights to enjoy legal capacity under Article 12 of the UN Convention on the Rights of Persons with Disabilities.
At the moment, the MCA 2005 is out of step with the UN Convention on the Rights of Persons with Disabilities, and out of step with international moves to bring disability law into alignment with that convention. The UK is a signatory to the Convention, and has ratified it and is therefore bound by its provisions. If a principled stance is being taken that the Government do not believe that our legislation is incompatible with the Convention (they have been told it is, by the Committee on the Rights of Persons with Disabilities, and by many legal academics and practitioners working in this field), then they need to say so, and I think they need to carefully explain why. If not, then why not take this rare opportunity to amend mental capacity law to increase protection of disabled people’s rights and empower them to get the support they require to make and influence all kinds of decisions in and about their lives?
Intransigence
A good deal of the debate was, again, focused on the proposed role for care home managers in the new Liberty Protection Safeguards. I noted my concerns about this back in July, and I’m sorry to say that the debate so far has done little to suggest to me that the concerns I have, which are shared by many in the care sector, are being taken seriously by the Government. They are, however, being taken very seriously indeed by many Peers, for which we should all be very grateful.
Yet, I’m still concerned about the conflict of interest inherent in private providers (whether for profit or not) being involved in the authorisation of deprivations of liberty in their care homes. I’m still concerned about the huge costs of implementing this framework in the care sector, and where the money to pay for it will come from (self-funders? Local authority social care budgets? Care home profits?). I’m still concerned about the paperwork burden on care home managers, who told me in the Everyday Decisions project that the increasing paperwork demands on them can get in the way of ensuring that their service provides the best possible care and support to their service users. I’m still deeply troubled about the lack of space in this proposal for consideration of less restrictive alternatives. I’m concerned about a lot of things.
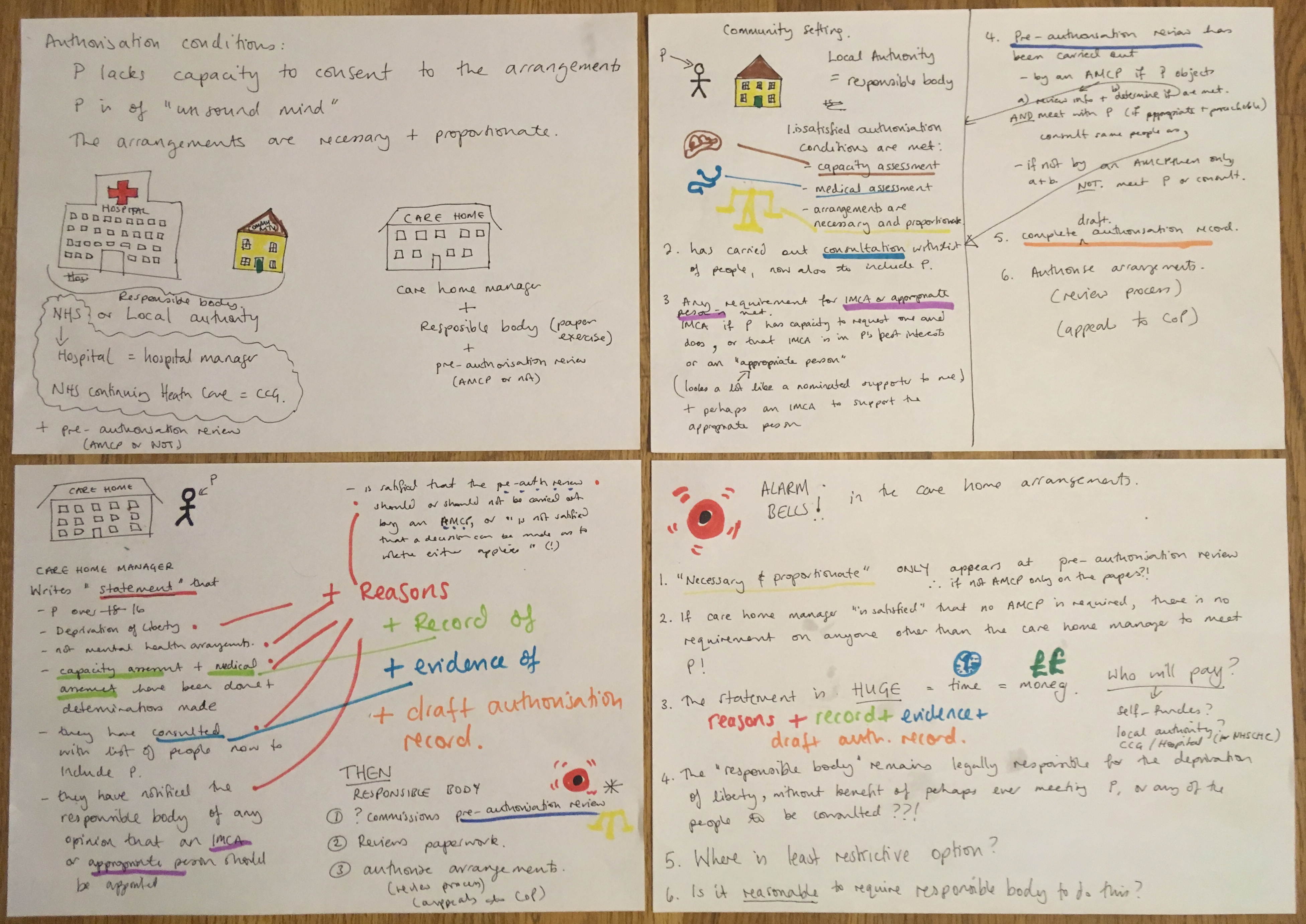
There have been some misunderstandings in relation to this issue, and I’m really not sure that the ‘flowchart’ provided by the minister makes it all that much clearer (please note that I am not claiming that my own notes, reproduced above, are helpful either). My reading of the text of the schedule, which will be the source of the law in this area irrespective of what is placed in the (not yet written, and not law) Code of Practice, is as follows:
If the person is to live in a care home, the care home manager will prepare a statement that:
- the capacity and medical assessments required under Article 5 ECHR (which can be pre-existing assessments) have been carried out;
- they have consulted with the required list of people (now to include the cared- for-person);
- they have notified the responsible body if an IMCA or appropriate person should be appointed;
- sets out their decision whether an Approved Mental Capacity Professional (AMCP) or someone who is not an AMCP should carry out the pre-authorisation review;
- gives reasons and evidence for all of these things.
The Care Home Manager will then draft the authorisation record and send the statement, evidence and record of the assessments to the responsible body. The responsible body (local authority or CCG) who can authorise the arrangements if the pre-authorisation review suggests that either the authorisation conditions are met (if conducted by an AMCP), or that it is reasonable for the responsible body to conclude that the authorisation conditions are met (if not conducted by an AMCP).
It is not entirely clear to me, from the face of the schedule, who would commission the pre-authorisation review, or when. It is also not clear from the face of the schedule who would do it if that review was not to be carried out by an AMCP, and what training or qualifications they would have to do so. I also find it most puzzling why it is only if the care home manager “is satisfied” that an AMCP should carry out the pre-authorisation review that there is actually any requirement for any person outside of that care home to meet the cared for person and talk to them about their wishes. Finally, I cannot see anywhere in that schedule a requirement for anyone to explore less restrictive alternatives under principle 5 of the MCA. I know that the principles will carry through as this is an amendment bill, not a new MCA, but I still think that serious consideration always needs to be given to the least restrictive alternative when we are thinking about depriving people of their liberty, and so it would make sense to be explicit about this here.
In summary: it is not clear and I am concerned. Reform is needed, and urgently because there are 125,000 people in the backlog of DoLS applications. That is over a hundred thousand intellectually disabled people who are currently sitting in the Bournewood Gap: lacking the capacity to consent to their care and treatment arrangements, under continuous supervision and control, not free to leave, and without any independent review of their situation. But we need to get this reform right, and the Government need to listen to those who seek a different approach than this complex, confusing and concerning model.